


Chronic constipation is one of the most common gastrointestinal disorders worldwide, yet millions of people suffer in silence, uncertain whether what they experience is “normal” or something that requires attention. According to a large systematic review published in The American Journal of Gastroenterology, chronic constipation affects roughly 14% of adults globally, with rates consistently higher in women and in older adults.[1]
Unlike an occasional bout of sluggish digestion, chronic constipation is a persistent condition defined by specific diagnostic criteria. It can significantly reduce quality of life, cause physical discomfort, and in some cases signal an underlying medical condition that needs treatment.
This guide covers what chronic constipation actually is, what causes it, how doctors diagnose it, what treatments are supported by clinical evidence, and how to prevent it from recurring. Every recommendation is backed by peer-reviewed research.
Key Takeaways
- What counts as “chronic”: symptoms most days for 3+ months, with onset at least 6 months earlier (the Rome IV criteria) — not just a few days of being backed up.
- Most common causes: low fiber and fluid intake, inactivity, certain medications (opioids, iron, some antidepressants), and ignoring the urge to go. Often no single cause is found.
- First steps that help most people: more fiber (25 g/day for women, 38 g/day for men), more water, regular movement, and not delaying bathroom trips.
- When to see a doctor: symptoms lasting more than 3 weeks, blood in the stool, unexplained weight loss, severe pain, or a significant change in bowel habits after age 50.
- Medical emergency: if you can’t pass any stool or gas at all, along with worsening bloating or pain, this could be fecal impaction — seek care promptly rather than trying home remedies first.
- If diet and lifestyle aren’t enough: bulk-forming or osmotic laxatives are the usual next step, with prescription options and biofeedback available for cases that don’t respond.
At a Glance: Best OTC Options for Chronic Constipation Relief
If diet and lifestyle changes alone aren’t enough, here are the most evidence-backed over-the-counter options to discuss with your doctor:
- Best for daily long-term fiber support: Metamucil Psyllium Fiber Powder — bulk-forming, builds regularity over 1-2 weeks, safe for daily use, the most studied fiber supplement for chronic constipation
- Best for gentle, predictable osmotic relief: MiraLAX Polyethylene Glycol 3350 Powder — draws water into the colon, works in 1-3 days, no cramping, well-tolerated for short-term use
- Best for faster saline-osmotic relief: Phillips’ Milk of Magnesia Liquid Laxative — stimulant-free and cramp-free, works in 30 minutes to 6 hours, the #1 milk of magnesia brand for over 150 years, avoid if you have kidney problems
- Best probiotic to support gut regularity long-term: Align Probiotic Supplement — contains Bifidobacterium 35624, a well-studied strain for digestive regularity
1. What Is Chronic Constipation?
Chronic constipation means ongoing trouble with bowel movements — they come too rarely, are hard to pass, or leave you feeling like you haven’t fully emptied your bowels. The word “chronic” is critical here. Almost everyone experiences brief episodes of constipation due to travel, dietary changes, or stress. Chronic constipation is different: it is recurring, it lasts for months, and it does not resolve on its own without intervention.
The most widely accepted clinical definition comes from the Rome IV diagnostic criteria, established by an international panel of gastroenterologists and updated in 2016. According to Rome IV, chronic constipation is present when a patient has experienced at least two of the following symptoms for the past 3 months, with symptom onset at least 6 months before diagnosis:[2]
- Straining during more than 25% of bowel movements
- Lumpy or hard stools (Bristol Stool Scale Type 1 or 2) in more than 25% of bowel movements
- A feeling of not fully emptying the bowels in more than 25% of bowel movements
- A feeling of blockage in the rectum or anus in more than 25% of bowel movements
- Needing to use your hands to help pass stool in more than 25% of bowel movements (for example, pressing on the abdomen or perineum, or removing stool manually)
- Fewer than 3 unassisted, complete bowel movements per week
Importantly, loose stools are rarely present without the use of laxatives, and there are insufficient criteria for a diagnosis of irritable bowel syndrome (IBS).
It is worth noting that “normal” bowel movement frequency varies widely. A classic, widely cited study found that going anywhere from 3 times a day to 3 times a week falls within a normal range for most healthy adults.[3] This is why the Rome IV criteria place equal weight on stool consistency, straining, and feelings of incomplete emptying — not just frequency alone.
2. How Common Is Chronic Constipation?
Chronic constipation is very common. Key statistics from peer-reviewed research include:
- It affects an estimated 14% of adults globally, with rates increasing with age and varying by region.[1]
- In the United States, constipation accounts for an estimated 5.7 million healthcare visits per year, with direct medical costs of roughly $235 million annually.[4]
- Women are roughly twice as likely as men to develop chronic constipation.[1]
- Despite its prevalence, many people never bring it up with a doctor and simply assume their symptoms are normal.
These numbers highlight why chronic constipation is considered a major public health issue, not just an inconvenient digestive complaint.

3. Symptoms of Chronic Constipation
The symptoms of chronic constipation go well beyond simply not going to the bathroom. People living with this condition frequently report a combination of physical and quality-of-life symptoms that can significantly interfere with daily activities.
Primary symptoms
- Fewer than 3 bowel movements per week on a consistent basis
- Hard, dry, or lumpy stools (Types 1 and 2 on the Bristol Stool Form Scale)
- Straining to pass stools
- Feeling of incomplete bowel emptying even after going
- Sensation of a blockage in the rectum or anus
- Needing to use your hands to help pass stool (for example, pressing on the abdomen or perineum)
Secondary and associated symptoms
- Abdominal bloating and distension
- Abdominal cramping or discomfort
- Nausea
- Loss of appetite
- Headaches
- Fatigue
- A general sense of feeling unwell
A study published in Alimentary Pharmacology & Therapeutics found that people with chronic constipation reported significantly lower quality-of-life scores than the general population — a reduction in well-being comparable in size to that seen with depression and chronic back pain.[5]
Stool form is one of the most reliable indicators. The Bristol Stool Form Scale classifies stools from Type 1 (separate hard lumps, like nuts) to Type 7 (watery, no solid pieces). Types 1 and 2 are associated with constipation, while Types 3 and 4 represent ideal stool consistency.

4. Causes and Risk Factors of Chronic Constipation
Chronic constipation rarely has a single identifiable cause. In most cases, multiple contributing factors work together to slow the movement of stool through the colon or make it harder to pass. Broadly, causes fall into two categories: primary (functional) causes and secondary (organic) causes, meaning constipation that is a side effect of another condition.
Dietary factors
A diet low in fiber is one of the most consistently identified dietary contributors to constipation. Dietary fiber adds bulk to stool and draws water into the colon, making stools softer and easier to pass. The average American consumes only about 15 grams of fiber per day, well below the recommended 25 to 38 grams.[6]
Inadequate fluid intake also plays a role. Without sufficient water, the colon absorbs more water from stool, making it harder and more difficult to pass. Diets high in processed foods, red meat, cheese, and refined carbohydrates are commonly associated with constipation, while diets rich in fruits, vegetables, legumes, and whole grains tend to promote regularity.
For more on dietary approaches, see our guide on the plant-based diet for constipation relief and our in-depth article on fiber foods and gut health.
Physical inactivity
Regular physical activity stimulates the muscle contractions that move stool through the colon. Research shows that sedentary individuals are significantly more likely to develop chronic constipation than physically active people.[7] Even moderate aerobic exercise, such as a 30-minute daily walk, may help reduce constipation symptoms.
Medications
Many commonly prescribed and over-the-counter medications can cause or worsen constipation as a side effect. The most frequently implicated include:
| Medication category | Examples |
|---|---|
| Opioid analgesics | Oxycodone, hydrocodone, morphine, codeine |
| Antidepressants | Tricyclic antidepressants (amitriptyline, nortriptyline) |
| Anticholinergics | Oxybutynin, tolterodine, diphenhydramine |
| Calcium channel blockers | Verapamil, nifedipine, diltiazem |
| Iron supplements | Ferrous sulfate, ferrous fumarate |
| Antacids | Aluminum-containing antacids (e.g., Maalox, Mylanta) |
| Antipsychotics | Clozapine, olanzapine |
| Diuretics | Furosemide (may cause dehydration and worsen symptoms) |
GLP-1 receptor agonists used for weight loss and diabetes management — such as semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) — have also been associated with constipation in clinical trials. These medications slow gastric emptying, which can reduce stool frequency. For more information on medications that contribute to constipation, see our guide on managing constipation through diet and lifestyle.
Hormonal and metabolic conditions
Several endocrine disorders are associated with slowed gastrointestinal motility (movement of food and stool through the gut):
- Hypothyroidism: An underactive thyroid slows down metabolic processes throughout the body, including gut movement. Constipation is one of the most common complaints in people with untreated hypothyroidism.[8]
- Diabetes mellitus: Nerve damage associated with long-standing diabetes (autonomic neuropathy) can impair gut motility. Diabetic gastroparesis (delayed stomach emptying) is one manifestation, but constipation is also common.[9]
- Hypercalcemia: Elevated blood calcium levels can reduce intestinal smooth muscle contractility.
- Pregnancy: Hormonal changes (elevated progesterone) and mechanical pressure from the growing uterus commonly contribute to constipation during pregnancy.
Neurological conditions
Neurological disorders that affect the nerves controlling the gut can cause constipation:
- Parkinson’s disease
- Multiple sclerosis
- Spinal cord injury
- Autonomic neuropathy (nerve damage affecting involuntary body functions)
Pelvic floor dysfunction
Dyssynergic defecation (also called anismus, or pelvic floor dyssynergia) happens when the pelvic floor muscles and anal sphincter don’t relax the way they should when you try to go — they tighten instead. This is thought to affect 25% to 50% of patients referred to specialist constipation clinics.[10]
Structural causes
In some cases, physical abnormalities of the colon or rectum may be responsible:
- Colorectal cancer or polyps causing obstruction
- Rectal prolapse (the rectum slipping out of place) or rectocele (a bulge of the rectum into the vaginal wall)
- Anal fissures (small tears that cause pain and avoidance of going)
- Strictures (narrowing) of the colon
If you are experiencing constipation alongside rectal pain, bleeding, or a feeling of incomplete emptying that does not respond to dietary measures, structural causes should be ruled out by a doctor.
Behavioral and psychological factors
Repeatedly ignoring the urge to go can, over time, reduce the body’s natural signal to use the bathroom. This is common in people with busy work schedules, limited bathroom access, or discomfort using public restrooms. Anxiety, depression, and stress also alter gut function through the gut-brain connection.
For a deeper dive into specific causes, see our article on why travel causes constipation.
5. Types of Chronic Constipation
Not all chronic constipation is the same. Gastroenterologists classify it into several subtypes, because understanding which type a patient has helps determine the most appropriate treatment.
Functional constipation (normal-transit constipation)
This is the most common type. Stool moves through the colon at a normal rate, but patients still feel constipated. Difficulty passing stool, hard stools, or a sensation of incomplete emptying are the predominant complaints. This subtype often responds well to dietary changes and fiber supplementation.
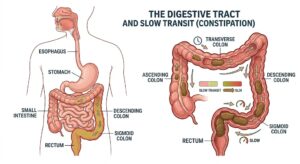
Slow-transit constipation (STC)
In slow-transit constipation, the colon moves stool more slowly than normal because the muscles of the colon are less active. This is more common in women and often begins in early adulthood. Patients typically report infrequent bowel movements (sometimes as few as once per week or less), little urge to go, and minimal improvement with dietary fiber alone. A colonic transit study — using swallowed markers tracked on X-ray, or a small wireless capsule — can confirm that movement through the colon is slower than normal.[11]
Dyssynergic defecation (outlet obstruction)
Also called obstructed defecation syndrome (ODS), this type involves a coordination problem with the muscles used to pass stool. A pelvic floor muscle (called the puborectalis) or the anal sphincter tightens instead of relaxing when you try to go, making it physically hard to pass stool regardless of how soft it is. Biofeedback therapy is the primary treatment.[10]
IBS with constipation (IBS-C)
IBS-C is characterized by constipation accompanied by abdominal pain or discomfort that is relieved by a bowel movement. This distinguishes it from functional constipation, where pain is not a core symptom. IBS-C has distinct Rome IV criteria and may respond to different treatments, including low-FODMAP dietary approaches and gut-directed medications.
Functional constipation vs. IBS-C at a glance
| Feature | Functional Constipation | IBS-C |
|---|---|---|
| Abdominal pain | Not a core symptom | Core symptom, typically eases after a bowel movement |
| Bloating | May occur | Very common |
| Rome IV classification | Diagnosed under its own criteria | Diagnosed under separate, distinct IBS criteria[12] |
| Main treatment focus | Fiber, hydration, osmotic laxatives | Low-FODMAP diet, gut-directed therapy, IBS-specific medications (e.g., linaclotide, tenapanor) |
Opioid-induced constipation (OIC)
This is a specific, increasingly prevalent subtype caused by opioid medications acting on receptors in the gut, which slows how quickly stool moves through the colon and dulls the urge to go. OIC is distinct from functional constipation and has dedicated prescription treatments (methylnaltrexone, naloxegol).
6. How Is Chronic Constipation Diagnosed?
Diagnosing chronic constipation involves a clinical history, physical examination, and sometimes diagnostic tests depending on symptom severity and the presence of alarm features.
Medical history and symptom assessment
A physician will ask about the frequency, consistency, and completeness of bowel movements; associated symptoms such as bloating, pain, and nausea; dietary habits; fluid intake; medications; medical history; and family history of colorectal disease. The Rome IV criteria are often used to formally establish the diagnosis.
Physical examination
A physical exam typically includes pressing on the abdomen (to detect masses, distension, or tenderness) and a digital rectal exam (DRE) — in which the doctor uses a gloved finger to check the muscle tone of the anus, feel for stool in the rectum, and look for signs of structural problems such as rectal prolapse or a rectocele.
Laboratory tests
Basic blood tests may be ordered to rule out secondary causes, including:
- Thyroid-stimulating hormone (TSH) to check for hypothyroidism
- Blood glucose or HbA1c for diabetes
- Serum calcium for hypercalcemia
- Complete blood count (CBC)
Colonoscopy
Colonoscopy is not routinely required for the initial evaluation of chronic constipation in younger patients without alarm features. However, it is recommended for patients over age 50 who are due for colorectal cancer screening, or for patients of any age with red flag symptoms such as rectal bleeding, unexplained weight loss, or a significant change in bowel habits.
Specialized motility tests
When first-line treatments fail or when the clinical picture suggests a specific subtype, further testing may include:
- Colonic transit study: You swallow tiny markers that show up on X-ray, or a small wireless capsule (SmartPill), so doctors can measure how long it takes contents to move through the colon.
- Anorectal manometry: A thin, pressure-sensing tube measures how well the muscles of the anus and rectum work together, which can reveal the coordination problem behind dyssynergic defecation.
- Defecography (proctography): An X-ray or MRI taken while you have a bowel movement, used to spot structural issues such as a rectocele or rectal prolapse.
- Balloon expulsion test: A simple office-based test where the patient attempts to expel a balloon filled with water from the rectum. Inability to expel suggests outlet obstruction.
7. When to See a Doctor
Many people manage mild constipation at home with dietary changes and over-the-counter remedies. However, certain symptoms should prompt a visit to a healthcare provider without delay.
See a doctor if you experience:
- Constipation that lasts more than 3 weeks despite dietary and lifestyle changes
- Blood in or on the stool (bright red or black tarry stools)
- Unexplained weight loss
- Severe or worsening abdominal pain
- Nausea and vomiting accompanying constipation
- A sudden, significant change in bowel habits (especially if you are over 50)
- Constipation that alternates with episodes of diarrhea
- A family history of colorectal cancer or inflammatory bowel disease
- Constipation that is not relieved by standard over-the-counter treatments
These are known as “alarm features” or “red flag symptoms” and warrant prompt evaluation to rule out colorectal cancer, intestinal obstruction, or other serious conditions.[13]
⚠️ When constipation becomes a medical emergency
If you cannot pass any stool or gas at all, have significant abdominal swelling, or notice watery stool leaking around what feels like a hard blockage, these can be signs of fecal impaction. This is not something to manage with home remedies or by waiting it out — it needs prompt medical evaluation, and in some cases urgent care. Contact a doctor or seek same-day medical attention.
8. Treatment Options: An Overview
Treatment for chronic constipation is highly individualized and typically follows a stepwise approach, starting with the least invasive options and escalating based on response.
The general treatment ladder looks like this:
- First line: Dietary and lifestyle modifications (fiber, hydration, exercise)
- Second line: Bulk-forming laxatives and osmotic laxatives
- Third line: Stimulant laxatives and other OTC remedies
- Fourth line: Prescription medications that increase fluid in the gut or stimulate gut movement
- Fifth line: Biofeedback therapy (for dyssynergic defecation), surgery (rarely)
The sections that follow cover each level of this treatment approach in detail.
9. Diet and Lifestyle Changes
Increase dietary fiber
Increasing fiber intake is often one of the first recommended approaches for managing constipation. A meta-analysis of randomized controlled trials found that dietary fiber significantly increased stool frequency and improved stool consistency in people with chronic constipation.[14]
The recommended daily fiber intake is 25 grams for women and 38 grams for men, though most people in Western countries fall well short of this. Fiber intake should be increased gradually to minimize bloating and gas, which are common when fiber is added too quickly to the diet.
High-fiber foods that may help include:
- Prunes and prune juice: One of the most evidence-supported natural remedies for constipation, with studies showing prunes may be more effective than psyllium at increasing stool frequency.[15]
- Kiwifruit: A randomized trial found that consuming 2 green kiwifruits per day was associated with significant improvements in constipation symptoms, bowel movement frequency, and stool consistency.[16] See our article on 2 kiwis a day for constipation.
- Legumes: Beans, lentils, chickpeas, and peas are high in both soluble and insoluble fiber.
- Whole grains: Oats, barley, whole wheat bread, and brown rice.
- Vegetables: Broccoli, spinach, carrots, Brussels sprouts.
- Fruits: Apples (with skin), pears, berries, figs.
For a research-backed overview of the most effective fruits, see our guide on the 10 best fruits for chronic constipation.
Stay well hydrated
Adequate fluid intake is essential for fiber to work effectively. When fiber absorbs water, it swells to form a soft, bulky stool. Without enough water, fiber can actually worsen constipation by creating a dense, hard mass. Aim for at least 6 to 8 cups (1.5 to 2 liters) of water per day, more in hot weather or during exercise.
Exercise regularly
A systematic review found that physical activity had a modest but significant benefit on constipation symptoms, particularly for increasing stool frequency.[17] Aerobic exercise (brisk walking, cycling, swimming) is most commonly studied and recommended. Even a 15 to 30 minute walk after meals can stimulate bowel activity through the body’s natural after-meal digestive reflex.
Don’t ignore the urge to go
Ignoring the urge to have a bowel movement repeatedly can reduce the body’s natural signal over time. When you feel the urge, try to use the bathroom within a reasonable time. Establishing a regular bathroom routine — such as sitting on the toilet for a few minutes each morning after breakfast (when the urge to go is naturally strongest) — can help retrain the bowel.
Optimize bathroom posture
Research has shown that adopting a squat-like position, with the knees raised above hip level (using a footstool), straightens the anorectal angle and may reduce straining and improve stool passage.[18]
For practical home remedies, see our article on 15 best natural laxatives for constipation and our guide to 5 morning habits to relieve constipation naturally.
10. Supplements That May Help
Psyllium husk
Psyllium is a soluble fiber derived from the seeds of Plantago ovata. It is one of the most studied supplements for constipation. A review published in The Journal of the American Association of Nurse Practitioners confirmed that psyllium may significantly improve stool consistency and frequency in adults with chronic constipation.[19] It should always be taken with plenty of water.
For guidance on when to take it, see our article on the best time of day to take fiber supplements.
Magnesium
Magnesium citrate and magnesium oxide work as osmotic agents, drawing water into the intestines and softening stool. A review published in Nutrients found that magnesium oxide supplementation may increase bowel movement frequency in people with functional constipation.[20] Note that people with kidney disease or impaired kidney function should consult a physician before using magnesium supplements, as impaired kidney function can reduce the body’s ability to excrete excess magnesium.
See our detailed guide to the 5 best magnesium supplements for constipation.
Probiotics
Probiotics are live bacteria that may support gut health by modulating the gut microbiome. A meta-analysis of 14 randomized controlled trials found that probiotics increased mean stool frequency by about 1.5 bowel movements per week and reduced gut transit time by about 12 hours compared with placebo.[21] Strains with the most evidence include Bifidobacterium lactis, among others.
For an in-depth review of the evidence, see our article on can probiotics help constipation, and for product recommendations, our guide to the 9 best probiotic supplements for 2026.
Natural laxatives
Several plant-based remedies have demonstrated efficacy in clinical research. Our comprehensive article on the 15 best natural laxatives for constipation covers these in detail.
11. Medications for Chronic Constipation
When dietary changes and over-the-counter supplements are insufficient, a physician may recommend or prescribe medications. These fall into several categories based on how they work.
Over-the-counter laxatives
| Type | Examples | How they work | Onset |
|---|---|---|---|
| Bulk-forming | Psyllium (Metamucil), methylcellulose (Citrucel) | Add bulk and water to stool | 12–72 hours |
| Osmotic | Polyethylene glycol (MiraLAX), lactulose, magnesium citrate | Draw water into the colon | 1–3 days |
| Stimulant | Senna (Senokot), bisacodyl (Dulcolax) | Stimulate intestinal contractions | 6–12 hours |
| Stool softeners | Docusate sodium (Colace) | Allow water and fats to mix with stool | 1–3 days |
| Lubricant | Mineral oil | Coats stool to ease passage | 6–8 hours |
Important note on stimulant laxatives: Senna and bisacodyl are generally intended for short-term relief. Using them daily without medical supervision for extended periods may lead to dependence and could reduce the colon’s ability to function without stimulation. If you find yourself reaching for a stimulant laxative every day, discuss longer-term options with your doctor.
For a detailed comparison of OTC products, see our guide to the best OTC laxatives for constipation.
Prescription medications
When OTC laxatives provide inadequate relief, several FDA-approved prescription options are available for chronic constipation:
| Medication | Mechanism (simplified) | Approved for | Most common side effect |
|---|---|---|---|
| Linaclotide (Linzess) | Pulls fluid into the intestines via gut-wall receptors; speeds transit[22] | Chronic idiopathic constipation (CIC), IBS-C | Diarrhea |
| Plecanatide (Trulance) | Works the same way as linaclotide | CIC | Diarrhea |
| Lubiprostone (Amitiza) | Opens a chloride channel in the gut lining to draw in fluid[23] | CIC, IBS-C (particularly in women) | Nausea |
| Prucalopride (Motegrity) | Stimulates serotonin receptors to speed colon movement | CIC, particularly slow-transit constipation | Headache, abdominal pain |
| Tenapanor (Ibsrela) | Blocks a gut transporter (NHE3) so less fluid is absorbed from the intestines | IBS-C | Diarrhea |
Side effects listed are the most frequently reported in clinical trials; this is not a complete list. Always review the full prescribing information with your doctor or pharmacist, since individual response and tolerability vary.
For more on this medication, see our article on prucalopride for chronic constipation.
Biofeedback therapy
For patients with dyssynergic defecation, biofeedback therapy is considered the treatment of choice. It uses sensors to help patients learn to relax their pelvic floor muscles and coordinate the muscles used to pass stool. Multiple randomized trials have confirmed its superiority over laxatives for this specific subtype of constipation.[10]
12. Complications of Untreated Chronic Constipation
Chronic constipation that is not adequately managed can lead to a range of complications.
Hemorrhoids
Straining during bowel movements increases pressure in the veins around the anus and rectum, causing hemorrhoids (enlarged veins). Hemorrhoids are one of the most common complications of chronic constipation and affect millions of people globally. See our article on the 10 best natural ways to relieve hemorrhoids and constipation.
Anal fissures
Hard, large stools can tear the lining of the anus (anal fissure), causing pain, bleeding, and spasm of the anal sphincter. Fissures may create a cycle of avoidance that worsens constipation.
Fecal impaction
In severe cases, stool can accumulate and become an immovable mass in the rectum (fecal impaction). This is a medical emergency that may require manual removal or enema treatment under medical supervision. It is particularly dangerous in elderly patients and individuals with neurological conditions. (See the emergency callout in Section 7 for warning signs.)
Rectal prolapse
Chronic straining can weaken the muscles and ligaments supporting the rectum, causing part of the rectum to protrude outside the body. This requires medical or surgical correction.
Reduced quality of life
As noted earlier, chronic constipation has a well-documented negative impact on quality of life, affecting work productivity, social functioning, sleep, and mental health.[5]
13. Prevention Strategies
Many cases of chronic constipation are preventable through sustainable lifestyle habits. Evidence-based prevention strategies include:
Eat a high-fiber diet consistently
Aim for 25 to 38 grams of fiber per day from whole food sources (fruits, vegetables, legumes, whole grains). Consistency matters more than occasional high-fiber meals. Include a variety of both soluble fiber (oats, beans, apples, psyllium) and insoluble fiber (wheat bran, vegetables, whole grains).
Drink adequate fluids daily
Water is the best choice. Caffeinated beverages (coffee, tea) may have a mild stimulant effect on the bowel for some people, which is generally fine in moderation. Alcohol and excess caffeine can contribute to dehydration and should be consumed with care.
Stay physically active
Regular moderate exercise is associated with a reduced risk of constipation. Even a 20 to 30 minute daily walk is enough to support healthy bowel motility for most people.
Establish a bowel routine
The urge to go is naturally strongest shortly after meals, especially after breakfast. Try sitting on the toilet for 5 to 10 minutes after your morning meal, whether or not you feel an urge. Do not strain. Over time, this can help establish regularity.
Listen to your body’s signals
Respond to the urge to go as promptly as reasonably possible. Repeatedly putting it off can reduce your body’s sensitivity to that signal over time.
Review your medications
If you take any of the medications listed in Section 4 and experience constipation, discuss alternatives with your doctor. Never stop a prescribed medication without medical advice, but your doctor may be able to switch you to a constipation-neutral alternative.
Manage stress
The gut and brain are closely connected. Chronic stress, anxiety, and depression can disrupt bowel function. Mind-body practices such as yoga, mindfulness, and cognitive-behavioral therapy may help manage both psychological stress and its gastrointestinal effects.
14. Chronic Constipation in Special Populations
Older adults
Constipation becomes significantly more prevalent with age, affecting up to one-third of adults over 60. Contributing factors include reduced physical activity, lower dietary fiber and fluid intake, taking multiple medications, reduced gut motility with aging, and other coexisting conditions. Management principles are similar to the general population, but extra care is needed to avoid complications like fecal impaction and to monitor for drug interactions.
Pregnant women
Constipation affects up to 40% of pregnant women, primarily due to elevated progesterone slowing intestinal motility, iron supplement use, and physical pressure from the growing uterus. Safe first-line interventions include dietary fiber and increased hydration. Psyllium and osmotic agents such as lactulose and polyethylene glycol are generally considered safe during pregnancy, but any medication use should be discussed with an obstetric provider.
Children
Functional constipation is one of the most common gastrointestinal complaints in children, estimated to account for 3 to 5% of pediatric outpatient visits.[24] Behavioral factors (withholding, toilet anxiety), dietary changes around weaning, and toilet training often play major roles. Polyethylene glycol is the best-studied and most commonly recommended treatment for pediatric constipation.
People with IBS-C
IBS with constipation requires careful differentiation from functional constipation, as abdominal pain is a prominent feature and treatment approaches differ (see the comparison table in Section 5). Low-FODMAP dietary interventions, gut-directed cognitive behavioral therapy, and medications such as linaclotide, plecanatide, or tenapanor may be beneficial for IBS-C specifically.
15. Frequently Asked Questions
What is the Rome IV definition of chronic constipation?
Rome IV defines chronic constipation as having at least two of the following symptoms for the last 3 months, with onset at least 6 months before diagnosis: straining in more than 25% of bowel movements, lumpy or hard stools in more than 25% of bowel movements, a feeling of incomplete emptying in more than 25% of bowel movements, a feeling of anorectal blockage in more than 25% of bowel movements, needing to use your hands to help pass stool in more than 25% of bowel movements, and fewer than 3 spontaneous bowel movements per week. Loose stools are rarely present without laxative use.
How long does constipation have to last to be considered chronic?
Constipation is generally considered chronic when symptoms persist for at least 3 months. The Rome IV criteria require that symptoms have been present for 3 or more months, with initial onset at least 6 months before diagnosis. Brief bouts of constipation lasting a few days are common and usually self-limited; it is the persistent, recurring pattern that defines chronicity.
What are the most common causes of chronic constipation?
The most common causes include a low-fiber diet, inadequate fluid intake, physical inactivity, certain medications (opioids, antidepressants, calcium channel blockers, iron supplements, aluminum-containing antacids), hormonal changes, ignoring the urge to go, and underlying conditions such as hypothyroidism, diabetes, pelvic floor dysfunction, or IBS-C. In many cases no single cause is found, and the condition is classified as functional constipation.
When should I see a doctor for constipation?
See a doctor if constipation lasts more than 3 weeks, is accompanied by blood in the stool, unexplained weight loss, severe abdominal pain, nausea or vomiting, or if over-the-counter remedies fail to provide relief. Seek medical attention if you experience a sudden significant change in bowel habits after age 50, as this may warrant colorectal cancer screening. If you cannot pass stool or gas at all, this needs prompt evaluation, not home treatment.
Can chronic constipation be cured permanently?
Many cases improve significantly — especially when an underlying cause is identified and treated, symptoms may resolve completely. However, for people with functional or slow-transit constipation, long-term management rather than a permanent cure is often the more realistic expectation. Working with a gastroenterologist to find the right combination of strategies tends to produce the best outcomes.
What foods make chronic constipation worse?
Foods commonly associated with worsening constipation include those low in fiber: processed foods, red meat, dairy products (particularly cheese), fast food, fried foods, white bread, and refined grains. These foods slow digestive transit time or reduce stool bulk and water content. Replacing them with high-fiber whole foods, fruits, vegetables, legumes, and adequate hydration generally supports more regular bowel movements.
Is it safe to use laxatives for chronic constipation every day?
Bulk-forming laxatives such as psyllium are generally considered safe for daily use and are often the first-line recommendation. Osmotic laxatives like polyethylene glycol (MiraLAX) are also well-tolerated for extended use under medical supervision. Stimulant laxatives such as senna are generally intended for short-term use; regular daily use without medical guidance may lead to dependence over time. Always consult a healthcare provider before using any laxative on a long-term daily basis.
What’s the difference between functional constipation and IBS-C?
The key difference is pain. In functional constipation, abdominal pain is not a defining feature. In IBS-C, recurring abdominal pain that improves after a bowel movement is a core diagnostic criterion, alongside the constipation itself. Because of this, IBS-C often responds best to a different toolkit — low-FODMAP dietary changes, gut-directed therapies, and IBS-specific medications — rather than fiber alone.
Affiliate Disclosure: This article contains affiliate links. If you purchase through our links, we may earn a small commission at no extra cost to you. Our editorial recommendations are based on research and are never influenced by affiliate relationships.
Medical Disclaimer: The content on this page is intended for general informational purposes only and does not constitute medical advice. It is not a substitute for professional medical consultation, diagnosis, or treatment. Always seek the guidance of a qualified healthcare provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
References
- Suares NC, Ford AC. Prevalence of, and risk factors for, chronic idiopathic constipation in the community: systematic review and meta-analysis. Am J Gastroenterol. 2011;106(9):1582-1591. PMID: 21606976
- Mearin F, Lacy BE, Chang L, Chey WD, Lembo AJ, Simrén M, Spiller R. Bowel Disorders. Gastroenterology. 2016;150(6):1393-1407. PMID: 27144627
- Connell AM, Hilton C, Irvine G, Lennard-Jones JE, Misiewicz JJ. Variation of bowel habit in two population samples. Br Med J. 1965;2(5470):1095-1099. PMID: 5838411
- Martin BC, Barghout V, Cerulli A. Direct medical costs of constipation in the United States. Dig Dis Sci. 2007;52(6):1417-1426. PMID: 17274481
- Belsey J, Greenfield S, Candy D, Geraint M. Systematic review: impact of constipation on quality of life in adults and children. Aliment Pharmacol Ther. 2010;31(9):938-949. PMID: 20180788
- Dahl WJ, Stewart ML. Position of the Academy of Nutrition and Dietetics: Health Implications of Dietary Fiber. J Acad Nutr Diet. 2015;115(11):1861-1870. PMID: 26514720
- Dukas L, Willett WC, Giovannucci EL. Association between physical activity, fiber intake, and other lifestyle variables and constipation in a study of women. Am J Gastroenterol. 2003;98(8):1790-1796. PMID: 12907334
- Yaylali O, Kirac S, Yilmaz M, et al. Does hypothyroidism affect gastrointestinal motility? Gastroenterol Res Pract. 2009;2009:529802. PMID: 20224642
- Bytzer P, Talley NJ, Leemon M, et al. Prevalence of gastrointestinal symptoms associated with diabetes mellitus: a population-based survey of 15,000 adults. Arch Intern Med. 2001;161(16):1989-1996. PMID: 11525701
- Rao SS, Seaton K, Miller M, et al. Randomized controlled trial of biofeedback, sham feedback, and standard therapy for dyssynergic defecation. Clin Gastroenterol Hepatol. 2007;5(3):331-338. PMID: 17368232
- Bharucha AE, Pemberton JH, Locke GR 3rd. American Gastroenterological Association technical review on constipation. Gastroenterology. 2013;144(1):218-238. PMID: 23261065
- Ford AC, Moayyedi P, Lacy BE, et al. American College of Gastroenterology monograph on the management of irritable bowel syndrome and chronic idiopathic constipation. Am J Gastroenterol. 2014;109(Suppl 1):S2-S26. PMID: 25091148
- Ford AC, Moayyedi P, Lacy BE, et al. (as above), monograph section on alarm features. PMID: 25091148
- Yang J, Wang HP, Zhou L, Xu CF. Effect of dietary fiber on constipation: a meta-analysis. World J Gastroenterol. 2012;18(48):7378-7383. PMID: 23326148
- Attaluri A, Donahoe R, Valestin J, Brown K, Rao SS. Randomised clinical trial: dried plums (prunes) vs. psyllium for constipation. Aliment Pharmacol Ther. 2011;33(7):822-828. PMID: 21323688
- Gearry R, Fukudo S, Barbara G, et al. Consumption of 2 green kiwifruits daily improves constipation and abdominal comfort — results of an international multicenter randomized controlled trial. Am J Gastroenterol. 2023;118(6):1058-1068. PMID: 36537785
- Tantawy SA, Kamel DM, Abdelbasset WK, Elgohary HM. Effects of a proposed physical activity and diet control to manage constipation in middle-aged obese women. Diabetes Metab Syndr Obes. 2017;10:513-519. PMID: 29276399
- Sikirov D. Comparison of straining during defecation in three positions: results and implications for human health. Dig Dis Sci. 2003;48(7):1201-1205. PMID: 12870773
- Lambeau KV, McRorie JW Jr. Fiber supplements and clinically proven health benefits: how to recognize and recommend an effective fiber therapy. J Am Assoc Nurse Pract. 2017;29(4):216-223. PMID: 28252255
- Mori H, Tack J, Suzuki H. Magnesium oxide in constipation. Nutrients. 2021;13(2):421. PMID: 33525523
- Dimidi E, Christodoulides S, Fragkos KC, Scott SM, Whelan K. The effect of probiotics on functional constipation in adults: a systematic review and meta-analysis of randomized controlled trials. Am J Clin Nutr. 2014;100(4):1075-1084. PMID: 25099542
- Chey WD, Lembo AJ, Lavins BJ, et al. Linaclotide for irritable bowel syndrome with constipation: a 26-week, randomized, double-blind, placebo-controlled trial. Am J Gastroenterol. 2012;107(11):1702-1712. PMID: 22986437
- Johanson JF, Ueno R. Lubiprostone, a locally acting chloride channel activator, in adult patients with chronic constipation: a double-blind, placebo-controlled, dose-ranging study. Aliment Pharmacol Ther. 2007;25(11):1351-1361. PMID: 17509103
- Tabbers MM, DiLorenzo C, Berger MY, et al. Evaluation and treatment of functional constipation in infants and children: evidence-based recommendations from ESPGHAN and NASPGHAN. J Pediatr Gastroenterol Nutr. 2014;58(2):258-274. PMID: 24345831



")
")
