


“I am taking Laxido prescribed by my GP. She gave me 60 sachets, and at two a day it will take one month — but I am feeling better two weeks on, after nearly five years of misery. I tried everything: probiotics, prebiotics, Digestic, Rheal, Wild Dose, Milk of Magnesia, magnesium citrate, gummies, Biomel. They work for a day or two and then stop. Of course there are also prunes, prune juice, and so on…”— Sarah M. (Shared via reader feedback; name changed for privacy)
The $4 Billion Industry That Fails Millions
The testimony above was shared with us by Sarah, a reader who, like many of you, spent half a decade trapped in a cycle of hope and frustration. Her story is not unusual; it is, in fact, painfully common. Many people spend years struggling with fiber and probiotics not working for constipation, despite following every “natural” health trend and high-end supplement brand available.
According to research published in StatPearls (NCBI), approximately 15% of the US population suffers from chronic constipation. Globally, an estimated 12% of people report ongoing symptoms—with those in North America suffering at twice the rate of Europeans. This represents hundreds of millions of people dealing with a condition that significantly affects their quality of life, productivity, and mental health.
Yet despite this scale, chronic constipation is persistently misunderstood—both by sufferers and the wellness industry that profits from them. The global laxative market is worth billions, much of it spent on “natural” solutions like probiotic capsules, fiber gummies, and magnesium powders. While these products work well for occasional sluggishness, they often fail those with chronic, deep-seated issues.
It is a hard truth to swallow: When you find fiber and probiotics not working for constipation, the reason is almost always biological. It is rooted in which type of constipation you have, not in how many supplements you are taking.
In this article, we will use Sarah’s 5-year journey as a roadmap to explain the science of “Mechanism Mismatch.” You will learn why natural remedies fail specific categories of chronic sufferers, the exact science behind why osmotic solutions like Laxido (Macrogol 3350) succeed, and how to identify the right approach for your unique gut.
Understanding Why Chronic Constipation Is Not One Disease
Before examining why individual remedies fail, the most important thing to understand is that “constipation” is an umbrella term, not a single condition. Gastroenterologists recognise several distinct subtypes, each with fundamentally different causes — and critically, different treatment requirements.
The four major categories are:
- Normal-Transit Constipation (NTC): The colon moves at a normal speed, but the person perceives difficulty or infrequency. This is the most common form and is often related to dietary fiber intake, hydration, and stress. This is the category that responds well to fiber, hydration changes, and gentle probiotics.
- Slow-Transit Constipation (STC), also called Colonic Inertia: The colon moves too slowly because of impaired muscle or nerve function. Fiber, probiotics, and gentle herbal remedies typically fail here — and can sometimes make things worse. This is the most treatment-resistant form and is far more common than many people realise.
- Outlet Dysfunction / Dyssynergia (Obstructed Defecation): The colon transit may be fine, but the pelvic floor muscles fail to coordinate during defecation. No laxative addresses this — pelvic floor physiotherapy and biofeedback are the primary interventions.
- Irritable Bowel Syndrome with Constipation (IBS-C): Constipation driven by gut-brain communication dysfunction, often accompanied by abdominal pain, bloating, and alternating stool patterns.
Sarah’s profile — five years, every natural remedy tried, partial responses that fade within two days — is the textbook presentation of slow-transit constipation. Understanding why requires looking at the biology of how the colon actually moves stool.
The Biology Behind a Stuck Colon: Interstitial Cells of Cajal
Most people think of constipation as a simple plumbing problem. In reality, for those with slow transit, it is closer to an electrical problem.
The colon is not a passive tube. It contracts rhythmically, pushing waste toward the rectum through coordinated muscular waves called peristalsis. This coordination depends on specialised pacemaker cells embedded in the colon wall called Interstitial Cells of Cajal (ICC). These cells generate and transmit the electrical signals that trigger muscle contractions — in much the same way that the heart’s sinoatrial node triggers a heartbeat.
In patients with slow-transit constipation, research published in Gastroenterology (Lyford et al., 2002) found that ICC volumes were decreased by 40% to 100% throughout the colon compared to healthy controls. A separate study in the same journal (Wedel et al., 2002) confirmed that ICC numbers are significantly reduced in all layers of the colonic muscularis in STC patients. The myenteric plexus — the network of nerves that controls gut movement — also shows reduced ganglionic density in these patients.
This biological deficit is also why STC often runs in families, why it disproportionately affects women (hormonal differences affect ICC function), and why it becomes more severe with age as ICC numbers naturally decline further.
This is also why Sarah’s various products each worked for a day or two then stopped: each intervention produced a brief response in a system that could not sustain it.
Slow-Transit Issues: Why Fiber and Probiotics Not Working for Constipation in Chronic Cases
One of the most common reasons for fiber and probiotics not working for constipation is a condition called slow-transit constipation or colonic inertia. In these cases, the muscles of the colon move too slowly. When you add more fiber, you are simply adding more bulk to a system that isn’t moving, which often leads to more bloating and pain instead of relief.
Why Probiotics Don’t Work for Slow-Transit Constipation
Probiotics are live bacteria that, when consumed in sufficient quantities, can alter the composition of gut microbiota. There is genuine, peer-reviewed evidence that specific strains — particularly Bifidobacterium lactis and Lactobacillus casei Shirota — can modestly improve bowel movement frequency in people with functional constipation.
A 2017 meta-analysis published in Nutrients reviewed 23 randomised controlled trials and found that probiotics improve stool frequency by an average of 0.83 bowel movements per week in constipated adults. That is a real but clinically modest effect, and crucially, the heterogeneity among studies was very high — meaning the results varied enormously from person to person.
Here is why this matters for slow-transit sufferers specifically: Probiotics work through the microbiome. They influence fermentation, gas production, and the chemical environment of the gut. Some strains may reduce populations of methane-producing archaea (methanogens), which can slow transit — and in this indirect way, modestly accelerate movement.
But they cannot compensate for impaired ICC function. They cannot restore the electrical signalling system that drives peristalsis. They cannot regenerate depleted myenteric neurons. They adjust the bacterial ecology of a system — and if that system’s fundamental motor architecture is dysfunctional, no amount of bacterial adjustment will produce regular bowel movements.
The products Sarah tried — including branded probiotic blends like Biomel, Digestic, and Rheal — are real probiotic products with real bacterial content. The issue was never product quality. The issue was mechanism mismatch: these products were designed for a different type of gut problem.
 Related Read: 9 Best Probiotic Supplements 2026
Related Read: 9 Best Probiotic Supplements 2026The Fiber Paradox: How More Fiber Can Make Things Worse
Dietary fiber is the first-line recommendation for constipation in virtually every clinical guideline — and for the majority of people with normal-transit constipation or insufficient fiber intake, it works. The science is clear on this.
But for slow-transit constipation, fiber presents a genuine paradox. Here is the mechanism: Fiber adds bulk to stool and draws water into the colon. In a colon with normal transit speed, this bulk stimulates peristalsis (the stretch reflex) and the stool moves. In a colon with impaired ICC function and reduced peristaltic capacity, the same bulk sits in a sluggish system that cannot generate enough contractile force to move it. You have simply added more weight to a lorry with a flat tyre.
A review published in the World Journal of Gastroenterology examined 149 patients with chronic constipation treated with Plantago ovata (psyllium) fiber for six weeks. The result: 80% of patients with slow-transit constipation showed no improvement. A separate review concluded directly: “An increase in fiber intake in these patients will not result in a decrease in stool transit time. There is, in fact, a deleterious effect of increasing faecal load without effectively increasing evacuation.”
This explains an experience that many chronic constipation sufferers report: adding fiber supplements, eating more prunes and vegetables, and increasing wholegrains produces more bloating, gas, and abdominal discomfort — but no additional bowel movements. The prunes and prune juice that Sarah mentioned are particularly instructive here. Prunes contain both fiber and sorbitol (a naturally occurring osmotic compound), which is why they help some people. But for a severely slow colon, even sorbitol’s osmotic effect is too limited and too brief to overcome the underlying motility deficit.
Why Magnesium, Milk of Magnesia, and Gummies Stop Working After Two Days
Sarah’s experience with magnesium citrate, Milk of Magnesia, and fiber gummies follows a consistent pharmacological pattern that has a specific explanation.
Magnesium-based products (magnesium citrate, magnesium oxide, Milk of Magnesia) work as osmotic agents: they draw water into the bowel lumen by creating an osmotic concentration gradient. This water influx softens stool and stimulates movement. It works — initially.
The problem is that the body’s colon is extremely efficient at compensating for osmotic changes. When magnesium ions enter the colon lumen, the body responds by adjusting water reabsorption rates to maintain homeostasis. In people with normal colons, this compensation is incomplete, so the stool moves before full compensation occurs. In people with slow-transit colons — where water reabsorption is already maximised because stool sits for so long — the compensation can catch up more quickly, neutralising the effect.
Additionally, magnesium at typical OTC doses creates only a limited osmotic gradient. This is sufficient for occasional constipation. For a colon where stool may be sitting for 72–100 hours or more (when the normal transit time is 10–30 hours), the gradient dissipates before sufficient movement is achieved.
The same applies to many herbal laxatives (Wild Dose and similar products containing senna or cascara). Stimulant laxatives work by chemically irritating the nerve endings in the colon wall, triggering contractions. In a normal colon, this produces movement. In a colon with depleted ICC and reduced myenteric neurons, the stimulant produces a partial response — brief, incomplete, and diminishing with each use as the already-compromised nerve endings become further habituated to the stimulus.
This is why Sarah’s pattern — brief response, then nothing — is so consistent across such different product types. The pattern is not evidence of bad products. It is a diagnostic clue pointing to the same underlying problem.
📖 Related Read: 5 Best Magnesium Supplements for Constipation (2026 Review)
The Science of Osmotic Relief: How Macrogol / PEG 3350 Works Differently
Understanding why osmotic laxatives like Macrogol 3350 succeed where magnesium and stimulants fail requires appreciating a crucial mechanistic difference.
What Is Macrogol 3350?
Macrogol 3350 — sold as Laxido and Movicol in the UK, and as MiraLAX (PEG 3350) in the United States — is a polyethylene glycol (PEG) molecule. It is biologically inert: the body does not absorb it, metabolise it, or react to it immunologically. It passes through the entire gastrointestinal tract chemically unchanged.
Its therapeutic effect comes entirely from its physical chemistry. The long polymer chains of the PEG molecule form hydrogen bonds with water molecules, binding them and physically preventing the colon from reabsorbing them. This is a fundamentally different mechanism from magnesium salts (which create a reversible ionic gradient) or stimulant laxatives (which activate nerve endings).
⚙️ Mechanism Comparison:
Magnesium osmotics → Create an ionic gradient. The body compensates by adjusting water reabsorption. Effect fades as homeostasis is restored. Short-acting.
Stimulant laxatives (senna, bisacodyl) → Chemically irritate colonic nerves to force contractions. Effective acutely but causes cramping, and the already-depleted nerve population in STC patients becomes habituated rapidly.
Macrogol / PEG 3350 → Physically binds water molecules through hydrogen bonding at a molecular level. The body cannot “compensate” for this because it is not an ionic or chemical signal — it is a mechanical bond. As long as the PEG molecule is present in the colon, water remains bound to it. The effect does not habituate because there is no receptor or chemical pathway to habituate.
This is why Sarah noticed that magnesium worked for a day or two then stopped, while Laxido (Macrogol 3350) continued working — and why by week two she was experiencing sustained improvement after five years of failure.
What Happens Inside the Colon When You Take Macrogol
When a sachet of Laxido or a capful of MiraLAX is dissolved in water and consumed, the PEG molecules travel through the stomach and small intestine unchanged — they are too large to be absorbed. When they reach the colon, they are surrounded by the stool material that is accumulating there.
The PEG molecules begin binding water from the colonic environment, preventing the colon wall from reabsorbing it. This has two consequences:
First, the stool gradually softens. Hard, desiccated stool (Type 1 or Type 2 on the Bristol Stool Scale) absorbs the water that the PEG molecules have held in place, becoming progressively softer and more voluminous.
Second, as the softened stool expands and its water content increases, it exerts gentle mechanical pressure on the colon wall. Even in a colon with reduced ICC function and impaired peristalsis, sufficiently soft and bulky stool can eventually trigger movement through the remaining contractile machinery.
This is why Macrogol does not produce immediate results: it takes 1–3 days for the initial effect and, in severe chronic constipation where stool has been accumulating for weeks or months, it may take up to two full weeks before the accumulated backlog clears. This matches exactly what Sarah reported — feeling better in the second week.
📊 Clinical Evidence: A placebo-controlled, randomised multicentre trial (DiPalma et al., Am J Gastroenterol 2000; PMID: 10685748) found:
- Week 1: PEG group achieved 4.2 bowel movements per week vs. 2.9 for placebo (P<0.01)
- Week 2: PEG group 4.5 bowel movements per week vs. 2.7 for placebo (P<0.001)
- PEG group reported significantly less cramping, better stool consistency, and less straining
- No significant differences in laboratory values — confirming the safety profile
A comprehensive review of 21 clinical studies involving 1,949 patients concluded that PEG 3350 is safe and effective in treating chronic constipation in children and adults, including the elderly, across multiple clinical trials, with a safety profile comparable to that of placebo.
Laxido (UK) vs MiraLAX (US): Are They the Same?
Yes. Both Laxido and MiraLAX contain the same active ingredient — Macrogol 3350 / Polyethylene Glycol 3350 — at equivalent therapeutic doses. They are clinically interchangeable in terms of mechanism and efficacy. The differences are packaging, brand, and the fact that Laxido in the UK is typically available by prescription while MiraLAX in the US is available over the counter.
Sarah’s GP prescribed Laxido at two sachets per day — a dose appropriate for clearing chronic constipation. The standard OTC dose of MiraLAX is 17g (one capful) once daily, which is suitable for maintenance once the initial backlog has cleared. For severe chronic cases, a GP may recommend the higher dose that Sarah received.
Other UK brand names for Macrogol 3350 include Movicol, Molaxole, and Cosmocol. All are the same active molecule.
📖 Related Read: Best Laxative for Constipation from Iron Pills (2026 Guide)
Product Comparison: What Are the Options and How Do They Compare?
| Product / Type | Mechanism | Works for STC? | Habituation Risk | Side Effects |
|---|---|---|---|---|
| Probiotics (e.g. Biomel, Rheal, Digestic) | Microbiome adjustment | Rarely | No | Bloating possible |
| Psyllium fiber / Metamucil | Bulk-forming | Often worsens STC | No | Bloating, gas |
| Magnesium citrate / Milk of Magnesia | Osmotic (ionic gradient) | Brief effect only | Yes (rapid) | Diarrhoea, cramping |
| Herbal stimulants (senna, Wild Dose) | Nerve stimulation | Brief effect only | Yes | Cramping, dependency risk |
| Macrogol 3350 / PEG (MiraLAX, Laxido) | Osmotic (mechanical bond) | Yes — first line for STC | No | Bloating initially, mild |
| Lactulose | Osmotic (disaccharide) | Partial | Low | Gas, bloating |
| Bisacodyl (Dulcolax) | Stimulant | Brief effect | Yes | Cramping, urgency |
| Docusate (Colace) | Stool softener | Insufficient for STC | No | Minimal |
Note: “Works for STC” refers specifically to slow-transit constipation. All products listed have legitimate uses for other constipation types or severity levels.
Recommended Products (US Readers — For Maintenance Phase)
MiraLAX 45-Dose Powder (PEG 3350) — Best Value for Chronic Use ⭐⭐⭐⭐⭐
The 45-dose bottle provides a full six-week supply at the standard once-daily dose — sufficient to see meaningful results in chronic cases. Tasteless and grit-free, it dissolves completely in any beverage including coffee, tea, juice, or water. No sugar, gluten-free, stimulant-free, and preservative-free.
Who it’s for: Adults with chronic slow-transit constipation who have already tried and failed with fiber and probiotic approaches. For severe chronic cases, consult your GP about dosing before starting.
Amazon Basic Care ClearLax (Generic PEG 3350) — Best Budget Alternative⭐⭐⭐⭐
Identical active ingredient (PEG 3350, 17g per dose) to MiraLAX at a significantly lower price point. FDA-approved. Fine-texture powder that dissolves without grit or residue. An excellent option for those managing chronic constipation long-term under GP supervision who want to reduce ongoing costs without sacrificing efficacy.
Who it’s for: Readers who have confirmed PEG 3350 works for their specific constipation type and want a cost-effective ongoing supply. View on Amazon →
How to Determine What Type of Constipation You Have
Before trying any product, it is worth spending five minutes identifying which category of constipation most likely applies to you. This can save months or years of cycling through ineffective treatments.
Step 1 — Use the Bristol Stool Form Scale
The Bristol Stool Form Scale (BSFS) is a validated clinical tool that classifies stool into seven types based on shape and consistency. It is a reliable proxy for colonic transit time.
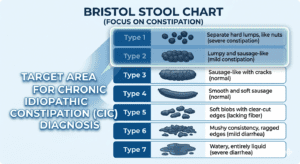
- Type 1: Separate hard lumps, like pebbles → Severely slow transit (>100 hours)
- Type 2: Sausage-shaped but lumpy → Slow transit (72–100 hours)
- Type 3: Sausage with cracks on surface → Slightly slow (48–72 hours), normal low end
- Type 4: Smooth, soft sausage or snake → Ideal transit (~30 hours)
- Type 5: Soft blobs with clear-cut edges → Fast transit, tendency toward loose
- Type 6: Fluffy pieces with ragged edges, mushy → Very fast transit, pre-diarrhoea
- Type 7: Entirely liquid, no solid pieces → Diarrhoea
If you consistently produce Type 1 or Type 2 stools, your transit is slow. Fiber supplementation alone is unlikely to resolve this — osmotic support is almost certainly needed. This is the profile that benefits from PEG 3350 / Macrogol.
If you produce Type 3–4 stools but still struggle to defecate despite normal-appearing stool, the issue may be outlet dysfunction or pelvic floor dyssynergia. This requires physiotherapy assessment, not laxatives.
If your stool type changes significantly day to day, correlating with stress, certain foods, or menstrual cycle, IBS-C is more likely. Dietary management (low-FODMAP approach) and certain probiotic strains are more appropriate here.
Step 2 — Self-Assessment Questions
Ask yourself these questions honestly:
Q: Does adding fiber (prunes, supplements, wholegrains) make your bloating significantly worse without increasing bowel movement frequency?
If YES → This points strongly toward slow-transit constipation.
Q: Do laxatives, magnesium, or herbal remedies work for 1–3 days then stop working?
If YES → The habituation pattern strongly suggests a motility disorder rather than a simple stool composition issue.
Q: Have you had these symptoms for more than three months, regardless of diet changes?
If YES → You are likely dealing with chronic functional constipation requiring medical assessment.
Q: Do you feel as though stool is “stuck” and complete evacuation never occurs, even when you eventually manage a movement?
If YES → This is a hallmark of slow-transit constipation or outlet dysfunction — both require specific intervention.
Q: Did your constipation begin or worsen after starting a new medication (opioids, antidepressants, iron supplements, calcium channel blockers)?
If YES → Medication-induced constipation is likely. Discuss with your prescriber — osmotic laxatives are first-line here, but the underlying medication must also be reviewed.
Step 3 — When to Move from OTC to Your GP
These are the signs that self-management with OTC products is insufficient and you should seek a GP appointment:
- You have experienced constipation for more than 3 months with no sustained relief from OTC options
- You notice blood in stool, unexplained weight loss, or severe abdominal pain alongside constipation
- You are over 50 and experiencing a new change in bowel habit (requires investigation to rule out structural causes)
- You have tried OTC Macrogol/PEG 3350 consistently for 2 weeks without meaningful improvement
- Your constipation requires increasing amounts of any laxative to maintain any effect
- You have constipation alongside symptoms suggesting IBS, hypothyroidism, diabetes, Parkinson’s, or multiple sclerosis
Sarah spent five years trying OTC options before seeing her GP. Her GP’s prescription of Laxido at two sachets per day — a therapeutic rather than maintenance dose — is what produced results. For severe slow-transit constipation, the OTC-recommended dose (one sachet or capful daily) is often insufficient. Only a prescribing GP can authorise the appropriate therapeutic dose.
Decision Framework: Which Treatment Matches Your Constipation Type?
| Your Pattern | Most Likely Cause | First Approach | If No Response |
|---|---|---|---|
| Occasional, responds to prunes/diet changes | Low-fiber diet, dehydration | Psyllium, increase water, exercise | N/A — may not be chronic |
| Type 1–2 always; fiber worsens bloating; remedies work 1–2 days then fail | Slow-transit constipation (colonic inertia) | See GP for Macrogol/PEG 3350 prescription dose | Specialist referral; colonic transit study |
| Stool looks normal (Type 3–4) but evacuation is incomplete, straining | Outlet dysfunction / pelvic floor dyssynergia | Pelvic floor physiotherapy assessment | Biofeedback therapy |
| Constipation alternating with loose stools; worse with stress; abdominal pain | IBS-C | Low-FODMAP diet; soluble fiber (psyllium); Bifidobacterium lactis probiotic | GP referral; prescription IBS-C medication |
| Constipation began with a specific medication | Drug-induced | Macrogol/PEG 3350 + discuss medication review with prescriber | Specialist review |
| Severe chronic: >3 months, all treatments failed | May require colonic transit study | Gastroenterology referral | Motility testing; possibly prescription secretagogues |
Five Lessons from Sarah’s Journey
Sarah’s five-year experience contains lessons that apply to anyone cycling through constipation treatments without lasting relief.
Lesson 1: Five years is too long to suffer in silence. There is a common tendency — particularly among people who consider themselves health-conscious — to avoid “medical” interventions in favour of natural approaches. But chronic constipation left unaddressed carries real health consequences. Persistent straining elevates the risk of haemorrhoids, anal fissures, rectal prolapse in severe cases, and — in truly refractory slow-transit constipation — dilatation of the colon (megacolon). Sarah’s five-year delay in seeking a GP prescription was not a personal failing; it reflects the messaging of an industry that positioned natural remedies as sufficient for all cases. They are not.
Lesson 2: “Natural” does not mean “appropriate for your specific condition.” Probiotics, prebiotics, magnesium, prunes, and herbal laxatives are all legitimate, evidence-backed interventions — for the right type of constipation. The products Sarah tried (Biomel, Rheal, Digestic, Wild Dose) are real products with real ingredients. The problem was never product quality. The problem was mechanism mismatch. These were the right tools for a different problem.
Lesson 3: Brief responses are diagnostic information, not proof of partial efficacy. When multiple products each work for a day or two then stop, this pattern itself tells you something clinically important: your colon can respond to chemical stimulation but cannot sustain that response. This is a hallmark of slow-transit constipation — not of products being “almost but not quite right.” Use this pattern to advocate for yourself with your GP.
Lesson 4: Consistency with the correct mechanism is everything. Sarah’s two-sachet-per-day Laxido routine works not because it is a stronger or more expensive product, but because the mechanism — sustained osmotic water-binding — matches her colon’s specific deficit. The water cannot be reabsorbed. The stool cannot dry out. Over weeks, the accumulated backlog clears, and the colon can begin functioning with reduced obstruction.
Lesson 5: The dose matters. The reason Sarah saw results with Laxido at two sachets daily but not with OTC magnesium or a standard single sachet is partly about dose. The therapeutic clearing dose for severe chronic constipation is often higher than OTC packaging suggests. Only a prescribing GP can authorise and monitor the appropriate dose for your specific situation.
Conclusion — Personalised Science Beats One-Size-Fits-All Advice
The global wellness industry has built a multi-billion-pound market on the premise that constipation is a universal problem with universal solutions: eat more fiber, take a probiotic, or try magnesium. For the majority of people with occasional or dietary-related constipation, this advice is sound.
However, for a significant minority suffering from slow-transit constipation, colonic inertia, or outlet dysfunction, this same advice is not just ineffective—it is the primary reason why you may find fiber and probiotics not working for constipation. This mismatch can keep people suffering for years while the right intervention sits just one GP appointment away.
Sarah’s story is a classic case study in what happens when the treatment mechanism is mismatched to the biological condition. She tried at least nine different products across five years of documented suffering. None were fraudulent; all had clinical evidence behind them. But none addressed her actual problem: a colon with impaired ICC function and depleted myenteric neurons. This was a structural inability to maintain movement that no amount of fiber could fix, which is a common scenario when fiber and probiotics not working for constipation.
Once her GP identified the correct mechanism and prescribed Macrogol 3350 (Laxido) at a therapeutic dose, she experienced more improvement in two weeks than in five years of trying alone. The osmotic science provided the constant hydration her sluggish colon needed to finally move.
If you recognize yourself in Sarah’s story—the cycling through premium products, the brief hopeful responses, and the constant frustration of fiber and probiotics not working for constipation—the most important step you can take is not purchasing another supplement. Instead, make a GP appointment and specifically describe your pattern: which products you have tried, how long each worked, and exactly what happened when they stopped.
This pattern is diagnostically informative. A knowledgeable GP or gastroenterologist will recognize it as a motility issue rather than a dietary deficiency. Finding the right mechanism, at the right dose, prescribed by the right clinician—that is what five years of searching finally achieved for Sarah.
Frequently Asked Questions
Q1: Why don’t probiotics work for my chronic constipation?
Probiotics work by adjusting gut bacteria, but they cannot compensate for impaired ICC (Interstitial Cells of Cajal) function or depleted myenteric neurons — the actual biological deficits in slow-transit constipation. Research shows probiotics improve stool frequency by less than one bowel movement per week on average, with enormous individual variation. For slow-transit sufferers, no bacterial adjustment produces the contractile force the colon itself cannot generate.
Q2: Can more fiber actually make constipation worse?
Yes — in slow-transit constipation. Adding fiber to a colon that cannot generate sufficient peristalsis increases the stool bulk without increasing transit speed. Research shows 80% of slow-transit patients show no improvement from additional fiber, and in some cases symptoms worsen. If fiber supplementation consistently makes your bloating worse without producing more bowel movements, this is diagnostically important — discuss it with your GP.
Q3: What is Laxido and is it the same as MiraLAX?
Yes. Both Laxido (UK) and MiraLAX (US) contain the same active ingredient: Macrogol 3350 / Polyethylene Glycol 3350. Both are osmotic laxatives that work by physically binding water in the colon and preventing its reabsorption. They are clinically equivalent. Movicol and Molaxole are additional UK brand names for the same molecule.
Q4: Why does MiraLAX / Laxido work when magnesium stops working?
Magnesium creates an ionic osmotic gradient that the body can partially compensate for within 1–3 days by adjusting water reabsorption rates. PEG 3350 / Macrogol works through a fundamentally different mechanism — it forms hydrogen bonds with water molecules at a molecular level, physically preventing reabsorption regardless of what the body’s regulatory systems do. There is no receptor pathway to habituate to this mechanical bond.
Q5: How long does Laxido / MiraLAX take to work?
For occasional constipation: 1–3 days. For chronic constipation with weeks or months of accumulated stool, meaningful improvement typically requires 1–2 weeks of consistent dosing. This matches Sarah’s experience. Do not judge efficacy in the first two to three days for chronic cases.
Q6: Is MiraLAX / Laxido safe for long-term use?
Under medical supervision, yes. A review of 21 clinical studies involving 1,949 patients found PEG 3350 to be safe with a profile comparable to placebo. The OTC label recommends up to 2 weeks without a doctor. For longer-term use — as in Sarah’s case with a GP prescription — ongoing monitoring is appropriate. Always follow your prescriber’s specific guidance.
Q7: Should I stop taking probiotics if they are not working?
Not necessarily — but do not continue indefinitely expecting them to resolve severe chronic constipation. Probiotics have genuine health benefits beyond constipation (immune function, general gut health). If you have slow-transit constipation, they will not fix that specific problem, but they may not be harming you either. Discuss with your GP whether to continue or discontinue based on your full picture.
Q8: I have tried Macrogol but it is not working — what next?
If you have taken Macrogol at the appropriate dose for at least two weeks without meaningful improvement, this is a signal for specialist referral. A gastroenterologist can perform a colonic transit study using radiopaque markers or a wireless motility capsule to objectively measure your transit time and identify the specific type and severity of dysfunction. From there, prescription secretagogues (linaclotide, lubiprostone) or other interventions may be considered.
Disclosure
ConstipationRelief.net is reader-supported. We may earn a commission from purchases made through our links, at no extra cost to you. This information is for educational use only and is not a substitute for professional medical advice. Reviewed for accuracy by Dr. ABM Sadikullah. Always consult your doctor before starting any new supplement, particularly if you have underlying health conditions.
References & Citations
- DiPalma JA et al. “A randomized, placebo-controlled, multicenter study of the safety and efficacy of a new polyethylene glycol laxative.” Am J Gastroenterol. 2000;95(2):446–450. PMID: 10685748. PubMed
- Dimidi E et al. “The effect of probiotics on functional constipation in adults: a systematic review and meta-analysis.” Am J Clin Nutr. 2014;100(4):1075–1084. PMID: 25099543. PubMed
- Lyford GL et al. “Pan-colonic decrease in interstitial cells of Cajal in patients with slow transit constipation.” Gut. 2002;51:496–501. BMJ Gut
- Wedel T et al. “Enteric nerves and interstitial cells of Cajal are altered in patients with slow-transit constipation and megacolon.” Gastroenterology. 2002;123(5):1459–1467. PMID: 12404220.
- Bharucha AE et al. “Idiopathic Slow Transit Constipation: Pathophysiology, Diagnosis, and Management.” Medicina. 2024;60(1):108. PMC10819559
- “Polyethylene Glycol 3350.” StatPearls, NCBI Bookshelf. NBK557652. NCBI
- Wegh CAM et al. “Probiotics, prebiotics, and synbiotics in chronic constipation.” Front Nutr. 2022;9:935830. Frontiers
- Bouhnik Y et al. “Macrogol 4000 without electrolytes in the symptomatic treatment of chronic constipation.” Drugs Context. 2018;7:212536. PMC6267542
- Oh SJ et al. “Chronic Constipation in the United States: Results From a Population-Based Survey.” Am J Gastroenterol. 2020;115(6):895–905.
- “Constipation.” StatPearls, NCBI Bookshelf. NBK513291. NCBI
- Magro DO et al. “Role of gut microbiota in functional constipation.” Gastroenterol Rep. 2021;9(5):392–401. Oxford Academic
- Voderholzer WA et al. “Clinical response to dietary fiber treatment of chronic constipation.” Am J Gastroenterol. 1997;92(1):95–98. PMID: 8995945.
")

: What Actually Works?")
")
")

{kind=link}
[…] you feel like you’ve tried every supplement with no luck, you aren’t alone. Read about when fiber and probiotics are not working for constipation and how Sarah found relief after a 5-year […]
[…] for constipation and bloating, strain identity is considered one of the most important factors. Probiotic effects are understood to be strain-specific — meaning the research on one strain does not automatically […]