


Sitting on the toilet but feeling like your poop is stuck and won’t come out can be uncomfortable, frustrating, and stressful. Many adults experience this problem at some point in their lives. If you are searching for answers to “Poop Stuck But Won’t Come Out?”, you may spend several minutes — or even longer — trying to pass stool, only to feel incomplete relief. This can cause bloating, abdominal pressure, and persistent discomfort.
In medical terms, this situation is often related to severe constipation or fecal impaction — a condition where stool remains in the large intestine for too long, becomes dry and hard, and can no longer pass naturally.
📋 What You’ll Learn in This Guide
- Why poop gets stuck — causes and physiology
- Occasional vs. severe constipation
- Immediate relief options — comparison table
- Step-by-step: what to do right now
- Correct toilet posture for easier bowel movements
- Foods, habits, and diet for long-term relief
- Safe laxatives — types, dosages, and side effects
- Special advice: children, pregnant women, older adults
- Complications of long-term constipation
- When to see a doctor — red flags
- Long-term prevention habits
- Frequently asked questions
Why Your Poop Gets Stuck But Won’t Come Out: Common Causes
The sensation that stool is lodged in the rectum and cannot be expelled is more than just an inconvenience — it is often an early sign of a serious condition known as fecal impaction. Understanding the physiological reasons behind this “stuck” feeling is essential for finding lasting relief.
1. Dehydration and Slow Colonic Transit
The primary function of the colon (large intestine) is to absorb water and electrolytes from digested food. Under normal circumstances, stool moves through the colon within 12 to 48 hours. When bowel motility slows, the colon absorbs an excessive amount of water from the waste material. According to the Mayo Clinic, this results in stool that is dry, dense, and difficult to pass. Dry stool creates significant friction against the intestinal walls, and natural peristalsis (the wave-like muscle contractions that move waste forward) cannot push the hardened mass forward — producing the classic “stuck” feeling.
2. Pelvic Floor Dyssynergia
Defecation is a highly coordinated neuromuscular event. A key muscle called the puborectalis wraps around the rectum like a sling and maintains the anorectal angle. During a normal bowel movement, the brain signals the puborectalis and external anal sphincter to relax, straightening the rectum and allowing stool to pass freely.
In some individuals, however, these muscles fail to relax — or may even contract paradoxically — during straining. This condition is known as pelvic floor dyssynergia. Research cited by Harvard Health Publishing indicates that this makes it feel as though the exit is blocked, even when the stool itself is not exceptionally hard. Chronic straining from this condition often leads to hemorrhoids and anal fissures over time.
3. Medical Conditions That Affect Gut Motility
Intestinal movement is governed by the autonomic nervous system and endocrine signals. Several clinical conditions can significantly disrupt this process:
- Irritable Bowel Syndrome (IBS-C): As noted by the NIDDK, IBS can cause irregular muscle contractions in the colon, leading to bouts of severe constipation.
- Diabetes and Autonomic Neuropathy: Long-term high blood sugar can damage the nerves controlling the digestive tract, resulting in a sluggish bowel.
- Hypothyroidism: According to the American Thyroid Association, an underactive thyroid slows the body’s entire metabolism, which directly reduces the speed of intestinal contractions.
4. Medication-Induced Constipation
Many common medications have a profound impact on bowel regularity. The Cleveland Clinic identifies several drug classes that frequently contribute to constipation or fecal impaction:
- Opioid pain medications: These bind to receptors in the gut, effectively slowing or halting the digestive process.
- Iron supplements: These increase stool density, making it darker, harder, and more difficult to pass.
- Certain antidepressants: Some psychiatric medications interfere with the chemical signals required for smooth muscle relaxation in the intestines.
- Anticholinergic drugs and anti-diarrheal medications: When overused, these can significantly reduce bowel motility.
5. Lifestyle Factors
Studies suggest that nearly 12–19% of adults worldwide experience chronic constipation. Common contributing factors include a low-fiber diet (particularly diets high in processed foods), insufficient daily fluid intake, a sedentary lifestyle, and regularly suppressing the urge to defecate. Experts from the Mayo Clinic and the NIDDK warn that untreated chronic constipation can lead to complications such as hemorrhoids, anal fissures, and other anorectal problems.
How Severe Constipation Differs from Occasional Constipation
Not all constipation is the same. While almost everyone experiences a backed-up feeling at some point, there is a significant clinical difference between a temporary bout of sluggishness and a chronic condition like fecal impaction.
Occasional Constipation (Temporary)
Occasional constipation is usually a short-term issue triggered by lifestyle changes. It typically lasts a few days and resolves with simple home remedies.
- Common triggers: Travel, a low-fiber meal, mild dehydration, or a change in daily routine.
- Symptoms: Hard stool requiring slight straining, mild bloating, and fewer than three bowel movements per week.
- Resolution: Usually responds to increased water intake, a short walk, or a single dose of over-the-counter fiber.
Severe or Chronic Constipation (Medical Concern)
Severe constipation, often termed Chronic Idiopathic Constipation (CIC), is defined by symptoms lasting three months or more. According to the American College of Gastroenterology, this condition frequently requires medical intervention because lifestyle changes alone often fail to provide adequate relief.
- Key indicators: Consistent straining, the need for manual maneuvers to pass stool, and a persistent sensation of incomplete evacuation.
- Risk of fecal impaction: If left untreated, severe constipation can progress to fecal impaction — where a large, hardened mass of stool becomes stuck in the rectum. This is a medical emergency capable of causing intestinal obstruction.
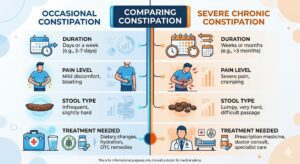
Quick Comparison: Occasional vs. Severe Constipation
| Feature | Occasional Constipation | Severe / Chronic Constipation |
|---|---|---|
| Duration | A few days | 3 months or longer |
| Frequency | Rare or tied to a specific event | Occurs consistently every week |
| Pain Level | Mild bloating or discomfort | Intense abdominal pain and cramping |
| Response to Home Remedies | Resolves with water and fiber | Often requires laxatives or enemas |
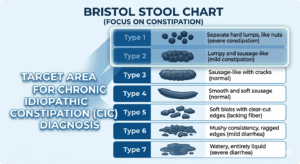
| Stool Consistency | Hard but manageable | Stone-like (Type 1 on Bristol Stool Chart) |
The Bristol Stool Chart: This validated medical tool classifies stool into 7 categories. Types 1–2 (hard, lumpy) indicate stool has spent too long in the colon. Types 3–4 are ideal. Types 5–7 indicate stool has passed through too quickly. Chronic Type 1–2 stools are the hallmark of the constipation described in this article.
Immediate Relief Options When Poop Is Stuck But Won’t Come Out
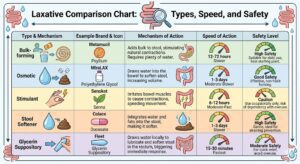
The table below compares the most widely used remedies by speed, purpose, and safety profile. Links connect to detailed in-site guides. Always consult your doctor or pharmacist before use.
| Type | Examples | Action Speed | Best Used For | Guide |
|---|---|---|---|---|
| Bulk-Forming Fiber | Psyllium Husk (Isabgol), FiberCon | 12–72 hrs | Relief without gas or bloating; suitable for daily use | Learn More |
| Osmotic Laxative | Polyethylene Glycol (MiraLAX), Magnesium Hydroxide | 6–48 hrs | Gentle, safe relief for chronic constipation | Learn More |
| Stimulant Laxative | Senna (Senokot), Bisacodyl (Dulcolax) | 6–12 hrs | Short-term emergency use only (max 7 days) | Learn More |
| Stool Softener | Docusate Sodium (Colace) | 12–72 hrs | Easier passage after surgery or when straining is painful | Learn More |
| Synbiotics | Probiotic + Prebiotic combined supplements | Weeks (long-term) | Restoring gut microbiome balance and bowel regularity | Learn More |
| Glycerin Suppository | Fleet Glycerin Suppositories | 15–30 mins | When stool is physically stuck at the rectal exit | Learn More |
What to Do Right Now: Step-by-Step Immediate Relief
When stool is stuck and won’t pass, guidelines from leading institutions like the Cleveland Clinic recommend the following evidence-based steps. The objective is to stimulate a bowel movement safely — never to force one.
1. Correct Your Posture First
Place a small footstool under your feet so your knees are elevated above your hips. This changes the anorectal angle from approximately 90 degrees to 35 degrees, straightening the rectal passage. This single change is often enough to allow stool to pass.
2. Drink Warm Water or Black Coffee
According to University of Michigan Health, warm liquids can initiate the gastrocolic reflex — a physiological response where drinking triggers the colon to contract and begin emptying its contents. Black coffee is particularly effective at stimulating colonic contractions. However, always follow coffee with a glass of plain water, as coffee has a mild diuretic effect that can promote dehydration if taken alone.
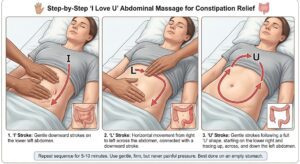
3. Perform the “I Love U” Abdominal Massage
When internal peristalsis is insufficient, external stimulation can help restart it. Using your fingertips, apply gentle but firm pressure and trace the following path on your abdomen — this pattern follows the path of the large intestine:
- “I”: Move downward along the left side of your abdomen.
- “L”: Move across the upper abdomen from right to left, then down the left side.
- “U”: Start at the lower right, move upward, cross to the left, then move downward.
Repeat slowly for 3–5 minutes. This can help push trapped gas and stool toward the rectum.
4. Use the “Blow Balloon” Breathing Technique
Avoid the Valsalva maneuver (holding your breath and bearing down hard). This can cause dangerous blood pressure spikes and worsen hemorrhoids. Instead, take a deep breath in, and as you push gently, exhale slowly through your mouth as if blowing up a balloon. This keeps the diaphragm relaxed and prevents the pelvic floor muscles from tensing involuntarily, allowing stool to pass naturally through the anal canal.
5.Use a Glycerin Suppository (If Stool Is at the Exit)
If the stool is close to the anal opening but too hard or large to pass on its own, a glycerin suppository can provide targeted relief. It works by lubricating the rectal area and drawing water into the rectum to soften the exterior of the stool. Effects typically occur within 15–30 minutes — a safer first option than a full enema for most adults.
⚠️ Know When to Stop
If you have tried these steps for more than 15–20 minutes without success, stop straining. Leave the toilet, move around, and try again later. Prolonged straining significantly increases the risk of anal fissures, hemorrhoids, and — in severe cases — rectal prolapse. Straining harder is never the solution.
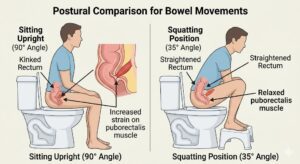
The Correct Toilet Posture That Makes Bowel Movements Easier
For decades, modern society has sat on toilets at a 90-degree angle — unaware that this position works against our anatomy. Research published by Harvard Health Publishing and endorsed by the Cleveland Clinic confirms that the standard toilet-sitting posture effectively “kinks” the digestive tract, creating a physical barrier to waste elimination.
Why the 90-Degree Position Fails
Inside the pelvis, the puborectalis muscle acts as a sling around the rectum. When you sit upright at 90 degrees, this muscle only partially relaxes, maintaining a sharp bend in the rectum known as the anorectal angle. Attempting to pass stool through this kinked passage requires significant straining — analogous to trying to run water through a bent garden hose. Over time, this repeated excessive straining leads to hemorrhoids and pelvic floor damage.
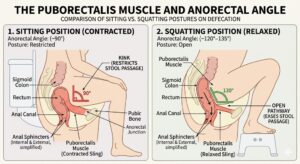
The 35-Degree Solution: Natural Squatting Position
The human body evolved to defecate in a squatting position. A study published in the journal Digestive Diseases and Sciences found that individuals who adopted a squatting posture passed stool significantly faster and with substantially less straining compared to those sitting upright. Elevating the knees above the hips shifts the body to approximately a 35-degree angle, allowing the puborectalis muscle to fully relax and straightening the anorectal passage completely.
How to Achieve the Correct Posture (Step-by-Step)
You do not need to replace your toilet. A simple modification is sufficient:
- Use a footstool: Place a small stool (such as a Squatty Potty or a basic plastic step-stool) in front of the toilet.
- Elevate your knees: Rest your feet on the stool so your knees are higher than your hips.
- Lean slightly forward: Lean your torso forward and rest your elbows on your knees. This further aligns the colon with the rectal passage.
- Keep your spine straight: Avoid rounding your back or slouching, which can misalign the internal anatomy.
Why This Matters for Long-Term Health
Consistently using the correct posture reduces the risk of several serious complications caused by chronic straining:
- Hemorrhoids: Swollen veins in the rectum caused by excessive downward pressure.
- Anal fissures: Small, painful tears in the lining of the anus from passing hard or oversized stools.
- Pelvic organ prolapse: A serious condition where pelvic organs (bladder, uterus, or rectum) shift out of their normal position due to years of excessive straining — particularly common in women.
Foods, Habits, and Diet That Naturally Improve Digestion
While immediate relief techniques address a current crisis, lasting digestive health comes from long-term, systemic changes. According to the World Gastroenterology Organisation (WGO), the foundation of healthy bowel movements is a consistent balance of fiber, hydration, and beneficial daily habits.
The Fiber Foundation: Soluble vs. Insoluble
Not all dietary fiber functions the same way. The body benefits from both types:
- Soluble fiber (oats, beans, apples, psyllium): Dissolves in water to form a gel that softens stool and slows digestion beneficially.
- Insoluble fiber (whole grains, vegetables, wheat bran): Adds bulk and accelerates stool movement through the intestines, acting like a natural broom.
The evidence-based recommendation is 25–35 grams of total fiber daily for adults. Most people currently consume significantly less than this target.

Hydration: The Colon’s Essential Lubricant
Fiber without adequate water is counterproductive — it can harden and worsen constipation. The large intestine’s primary job is to reabsorb water from waste material; dehydration causes it to extract too much, leaving stool hard and dry. Aim for 2–3 liters of fluid per day. A practical habit: drink a large glass of room-temperature water immediately upon waking to trigger the gastrocolic reflex and prepare the bowel for a morning movement.
Probiotics and Synbiotics for Chronic Constipation
Your gut is home to trillions of microorganisms (the gut microbiome) that play a critical role in digestion and bowel regularity. Clinical research increasingly supports the use of synbiotics — a strategic combination of a probiotic (live beneficial bacteria) and a prebiotic (the specific fiber that feeds those bacteria).
- Probiotic food sources: Yogurt (with live Bifidobacterium and Lactobacillus cultures), kefir, and sauerkraut.
- The synbiotic advantage: According to studies in the American Journal of Clinical Nutrition, synbiotics significantly increase weekly bowel movement frequency and improve stool consistency by accelerating colonic transit time — more effectively than probiotics alone.
Simple synbiotic food pairings to try at home:
- Yogurt + bananas or oats (live cultures paired with resistant starch)
- Kefir + chia seeds (potent live bacteria combined with mucilaginous fiber)
Leverage Your Gut’s Circadian Rhythm
The gut has its own internal clock and is most active in the morning, particularly in the 30–60 minutes following the first meal. Establish a consistent toilet routine — sit at the same time each morning, ideally 20–30 minutes after breakfast. Even if nothing happens immediately, this habit gradually trains the brain-gut connection to prepare the bowel at that time. Avoid heavy, high-fat meals late at night; late-night eating forces the digestive system to work when it should be resting and repairing.
Movement as a Natural Laxative
Physical activity increases blood flow to the GI tract and directly stimulates the smooth muscles that propel waste forward. Research indicates that as little as 20–30 minutes of brisk walking per day can significantly reduce colonic transit time. Consistent, moderate movement is sufficient — intense exercise is not required.
Top “Super-Mover” Foods for Digestion
- Prunes (dried plums): Rich in sorbitol — a naturally occurring sugar alcohol that acts as an osmotic laxative — and insoluble fiber.
- Chia seeds: Can absorb up to 12 times their weight in water, adding ideal bulk and softness to stool.
- Leafy greens (spinach, kale): Excellent sources of magnesium, which relaxes intestinal muscles and draws water into the colon.
- Papaya: Contains papain, a proteolytic enzyme that aids in breaking down proteins and supports overall digestive efficiency.
Safe Laxatives and Natural Remedies: Dosages and Side Effects
When lifestyle changes are insufficient to relieve a severe blockage, laxatives become a necessary tool. The American Gastroenterological Association (AGA) cautions that using the wrong type of laxative, or overusing any type, can lead to dependency and impaired bowel function. Understanding the categories and their appropriate use is essential for safe relief.
1. Osmotic Laxatives — Generally the Safest First Choice
Osmotic laxatives are the preferred first-line pharmacological treatment for chronic constipation. They do not force bowel contractions; they work by managing water balance in the colon.
- How they work: Draw water from surrounding tissues into the colon, softening stool.
- Common examples: Polyethylene Glycol (MiraLAX), Magnesium Hydroxide (Milk of Magnesia), Lactulose.
- Typical dosage (PEG / MiraLAX): 17 g of powder dissolved in 4–8 oz (120–240 ml) of liquid, once daily.
- Side effects: Bloating, gas, or mild abdominal cramping — particularly when first starting.
- Safety: Generally safe for longer-term use under medical supervision; not habit-forming.
2. Bulk-Forming Laxatives — Natural Fiber Supplements
These are concentrated forms of dietary fiber — the pharmacological equivalent of improving diet quality.
- Common examples: Psyllium husk (Isabgol / Ispaghula), Methylcellulose.
- Typical dosage (Psyllium husk): 1 tablespoon mixed thoroughly in a full glass (minimum 240 ml / 8 oz) of water, taken 1–3 times daily.
- Critical rule: Must always be taken with a full glass of water. Without adequate fluid, bulk-forming laxatives can cause a paradoxical physical blockage — worsening the original problem significantly.
- Side effects: Initial bloating or gas as the gut microbiome adjusts, typically resolving within 1–2 weeks.
3. Stimulant Laxatives — For Emergency or Short-Term Use Only
These are more aggressive and should be reserved for short-term emergency situations only.
- How they work: Irritate the bowel lining, stimulating muscular contractions that push stool toward the rectum.
- Common examples: Senna (Senokot), Bisacodyl (Dulcolax).
- Typical dosage (Senna): 8.6 mg to 17.2 mg once daily, usually at bedtime for a morning bowel movement.
- Side effects: Sharp stomach cramps, diarrhea, and electrolyte imbalance with prolonged use.
- Warning: Do not use for more than 7 consecutive days without medical supervision. Long-term use can cause laxative dependency — the colon becomes progressively less able to function independently.
4. Natural Kitchen Remedies
Several natural substances provide clinically meaningful relief before turning to pharmaceutical options:
- Prune juice: Contains sorbitol, a natural sugar alcohol with osmotic laxative properties. Starting dose: 120–240 ml (4–8 oz) in the morning.
- Castor oil: A potent natural stimulant laxative. Typical dose: 15 ml on an empty stomach. Avoid entirely during pregnancy — it can stimulate uterine contractions and risk premature labor.
- Aloe vera juice: Contains anthraquinones that stimulate gut motility. Typical dose: 60–120 ml (2–4 oz) daily. Use for short periods only, as high doses can cause electrolyte imbalances.
Laxative Comparison at a Glance
| Type | Examples | Speed of Action | Safety for Regular Use |
|---|---|---|---|
| Bulk-Forming | Psyllium Husk (Isabgol) | 12–72 hours | High — suitable for daily use |
| Osmotic | MiraLAX, Milk of Magnesia | 6–48 hours | High — safe under medical supervision |
| Stimulant | Senna, Bisacodyl | 6–12 hours | Low — short-term only (max 7 days) |
| Glycerin Suppository | Fleet Glycerin | 15–30 minutes | Medium — suitable for occasional use |
Special Advice for Children, Pregnant Women, and Older Adults
Constipation does not affect everyone in the same way. These three groups face unique physiological challenges. According to the American College of Gastroenterology, treating them requires careful consideration of both safety and effectiveness.
Children: Breaking the Withholding Cycle
Pediatric constipation is often as behavioral as it is physical. Children frequently resist having a bowel movement after one painful experience, creating a reinforcing cycle where delayed stool becomes larger, harder, and more painful.
- Dietary approach: Focus on “P” fruits — prunes, pears, and plums — which contain natural sorbitol. Ensure adequate water intake throughout the day, especially at school.
- Routine: Establish a consistent toilet-sitting habit. Have the child sit for 5–10 minutes after breakfast or dinner to leverage the body’s natural post-meal gastrocolic reflex.
- Critical warning: Do not give stimulant laxatives (senna or bisacodyl) to children without a pediatrician’s explicit prescription.
Pregnant Women: Managing the Progesterone Effect
Constipation affects an estimated 40% of pregnant women at some point. The primary cause is elevated progesterone, which relaxes intestinal smooth muscle and slows food transit. The growing uterus also places direct physical pressure on the colon.
- Recommended approach: Bulk-forming agents such as psyllium husk are the safest first-line option — they are not absorbed into the bloodstream and do not reach the fetus. Increasing daily walking and dietary fiber intake is also safe and effective.
- Critical warning: Avoid castor oil entirely during pregnancy — it can stimulate uterine contractions and potentially induce premature labor. Always consult your obstetrician or midwife before taking any laxative during pregnancy.
Older Adults: Addressing the Aging Digestive System
As we age, the digestive system naturally loses smooth muscle tone and nerve sensitivity. Medications commonly prescribed to older adults — including those for blood pressure, pain management, and depression — frequently list constipation as a side effect. Reduced mobility compounds the problem further.
- Recommended approach: Osmotic laxatives (such as MiraLAX) are considerably gentler on the aging gut than stimulant laxatives and are generally preferred in this population.
- Hydration strategy: The sensation of thirst diminishes significantly with age. Older adults should follow a proactive hydration schedule — drinking a small glass of water every 2 hours throughout the day, regardless of whether they feel thirsty.

Hidden Dangers: Complications of Long-Term Constipation
Ignoring chronic constipation is not merely uncomfortable — it can progress to serious medical conditions, including some that require surgical intervention:
- Hemorrhoids: Swollen, inflamed veins in or around the anus, caused by repeated excessive straining during bowel movements.
- Anal fissures: Small but painful tears in the lining of the anus, typically caused by passing very hard or large stools.
- Fecal impaction: When stool becomes so compacted and hardened in the rectum that it cannot be passed naturally, requiring manual removal by a medical professional or treatment with enemas. This can be a medical emergency if left untreated.
- Rectal prolapse: A condition where part of the rectum protrudes through the anus due to the weakening of supporting muscles and ligaments from years of chronic, excessive straining.
Red Flags: When to See a Doctor Immediately
Most constipation cases resolve with home management, but certain symptoms demand prompt medical evaluation. They may indicate a bowel obstruction, colorectal cancer, or another serious underlying condition. According to the American College of Gastroenterology, seek medical attention without delay if you experience any of the following:
🚨 Seek Medical Attention If You Notice:
- Blood in stool: Bright red blood on toilet paper or in the bowl, or dark, tarry stools (indicating possible internal bleeding higher in the GI tract).
- Unexplained weight loss: Losing weight without a dietary change while experiencing constipation.
- Severe, persistent abdominal pain: Sharp or cramping pain that does not resolve after a bowel movement, or that prevents you from standing upright.
- Thin, pencil-like stools: A persistent change to narrow stools can indicate a physical narrowing or blockage within the colon.
- Inability to pass gas: Combined with vomiting, severe bloating, and constipation, this is a potential sign of a complete bowel obstruction — a medical emergency requiring immediate care.
- Fever alongside constipation: May indicate an infection in the colon wall, such as diverticulitis.
- New constipation after age 50: A sudden change in bowel habits in adults over 50 warrants colonoscopic investigation to rule out colorectal cancer.
Long-Term Prevention: Four Foundational Habits
To avoid returning to the stuck-stool cycle, adopt these four habits consistently:
- The Fiber Rule: Aim for 25–35 g of dietary fiber daily from a variety of whole food sources — fruits, vegetables, legumes, and whole grains.
- The Hydration Habit: Drink a minimum of 2 liters of water per day. A practical strategy is one glass every 2 hours during waking hours.
- The Morning Ritual: Wake up, drink a glass of warm water, and take a 10–15 minute walk. This combination stimulates the gastrocolic reflex and gets the bowels moving before the day begins.
- Respond to Your Body’s Signals: Never ignore or suppress the urge to have a bowel movement. Delaying causes stool to remain in the colon longer, where more water is absorbed — making it progressively harder to pass.
📖 Continue Reading on ConstipationRelief.net
Frequently Asked Questions
Q1: Is it normal to have a bowel movement only three times a week?
Yes. According to the Mayo Clinic, normal bowel movement frequency ranges from three times a day to three times a week. Constipation is clinically defined as fewer than three bowel movements per week, particularly when accompanied by straining, hard stools, or a sense of incomplete evacuation.
Q2: Can I become dependent on laxatives if I use them too often?
It depends on the type. Stimulant laxatives (senna, bisacodyl) can cause dependency if used for more than seven consecutive days without medical oversight, as the bowel may become reliant on external stimulation. Bulk-forming (psyllium husk) and osmotic (polyethylene glycol) laxatives are generally safe for longer-term use under medical supervision and do not carry the same risk of dependency.
Q3: Does drinking coffee really help with constipation?
For many people, yes. Coffee stimulates colonic muscle contractions through a mechanism related to the gastrocolic reflex — the same reflex triggered by eating. However, coffee is also a mild diuretic. If you do not drink adequate water alongside it, the net effect on hydration could potentially worsen constipation over time. Drink a glass of water with your morning coffee to counteract this.
Q4: Why does constipation get worse when I travel?
This is commonly called “traveler’s constipation.” It occurs because travel disrupts your body’s circadian rhythm (internal clock), alters your normal diet, reduces physical activity, and often involves prolonged sitting. To minimize it, maintain your regular morning routine as closely as possible, stay well-hydrated during flights and long drives, and try to eat high-fiber foods even when traveling.
Q5: Are synbiotics better than regular probiotics for constipation?
Clinical evidence suggests that synbiotics (the combination of probiotics and prebiotics) are more effective for chronic constipation than probiotics alone. While probiotics introduce beneficial bacteria into the gut, synbiotics also provide the specific prebiotic fibers those bacteria need to survive stomach acid and thrive in the colon. This combination has been shown in multiple studies to more significantly improve colonic transit time and stool consistency.
Scientific Sources and References
This guide is based on peer-reviewed research and clinical guidelines from the following institutions:
- Harvard Health Publishing — The Lowdown on Laxatives
- Johns Hopkins Medicine — Constipation: What You Need to Know
- Cleveland Clinic — The Proper Way to Poop: Is Your Posture Correct?
- National Institutes of Health (NIDDK) — Treatment for Constipation
- American Journal of Clinical Nutrition — Probiotics and Synbiotics for Constipation Relief
- World Gastroenterology Organisation (WGO) — Global Guidelines on Constipation Management
- Mayo Clinic — Constipation: Symptoms and Causes
")


")
")

{kind=link}
[…] If the issue is stool that feels stuck and will not pass, this dedicated guide may help: Poop Stuck But Won’t Come Out. For older adults specifically, you can also explore immediate constipation relief strategies for […]
[…] explore natural fiber supplements for constipation, yoga poses that help with constipation, and what to do when stool will not pass for additional approaches you can combine with […]
[…] prebiotic, and synbiotic groups but not in placebo. If you’ve never seen this scale, our Bristol Stool Chart guide explains what each stool type […]